To be taken orally, independent of mealtime. If the tablets are taken on an empty stomach, the active substance is absorbed more rapidly. In this case, tablets should not be taken concurrently with dairy products or with mineral fortified drinks alone (e.g. milk, yoghurt and calcium fortified orange juice). However, dietary calcium as part of a meal does not significantly affect the absorption of ciprofloxacin. If the patient is unable to take tablets, because of the severity of the illness or for other reasons, it is recommended to commence the therapy with an intravenous form of ciprofloxacin. After intravenous administration the treatment can be continued orally.
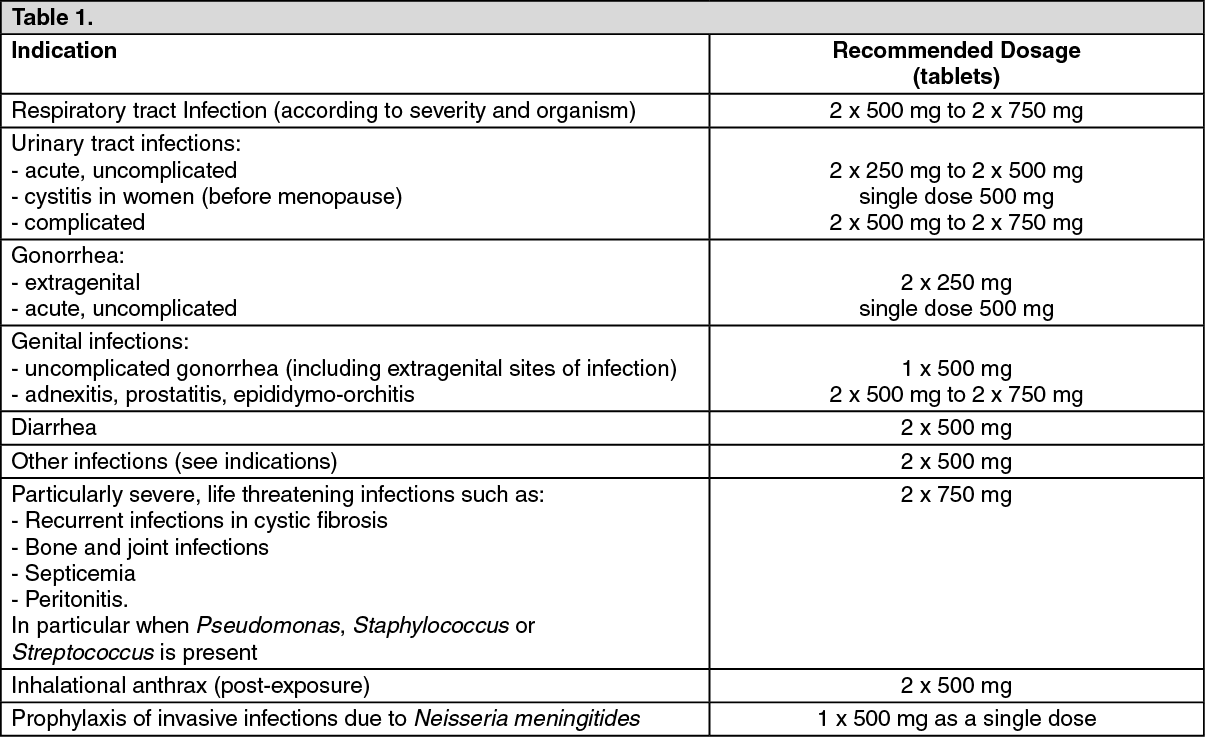
Adults: Unless otherwise prescribed, the following guideline doses are recommended; (See Table 1.)
 Click on icon to see table/diagram/image
Additional information on special patient population: Children and adolescents:
Click on icon to see table/diagram/image
Additional information on special patient population: Children and adolescents: Cystic Fibrosis: Clinical and pharmacokinetic data support the use of Ciprofloxacin in pediatric cystic fibrosis patients (aged 5-17 years) with broncho-pulmonary infections associated with
Pseudomonas aeruginosa infection, at a dose of 20mg/kg body weight oral twice daily with a maximum of 750mg per dose or 10mg/kg body weight intravenous three times daily with a maximum of 400mg per dose.
Complicated Urinary Tract Infections and Pyelonephritis: For complicated urinary tract infections or pyelonephritis the dose is 10mg/kg body weight oral twice daily to 20mg/kg body weight oral twice daily with a maximum of 750mg per dose or 6mg/kg body weight intravenous three times daily to 10mg/kg body weight intravenous three times daily with a maximum of 400mg per dose.
Geriatric patients (> 65 years): Elderly patients should receive a dose as low as possible depending on the severity of their illness and the creatinine clearance.
Patients with renal and hepatic impairment: Adults: Impaired renal function: Patients with creatinine clearance between 30 and 60mL/min/1.73m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9mg/100mL, the maximum daily dose should be 1000mg for oral administration or 800mg for an intravenous regimen.
Patients with creatinine clearance less than 30mL/min/1.73m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0mg/100mL, the maximum daily dose should be 500mg for oral administration (all formulations) or 400mg for an intravenous regimen.
Impaired renal function and hemodialysis: Patients with creatinine clearance between 30 and 60mL/min/1.73m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9mg/100mL, the maximum daily dose should be 1000mg for oral administration (all formulations) or 800mg for an intravenous regimen.
Patients with creatinine clearance less than 30mL/min/1.73m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0mg/100mL, the maximum daily dose should be 500mg for oral administration (all formulations) or 400mg for an intravenous regimen on dialysis days after dialysis.
Impaired renal function and continuous ambulatory peritoneal dialysis (CAPD): Addition of ciprofloxacin infusion solution to the dialysate (intraperitoneal): 50mg ciprofloxacin/liter dialysate administered 4 times a day every 6 hours.
Administration of ciprofloxacin film-coated tablets (oral) as 1 x 500mg film-coated tablet (or 2 x 250mg film-coated tablets).
Impaired liver function: No dose adjustment is required.
Impaired renal and liver function: Patients with creatinine clearance between 30 and 60 mL/min/1.73m
2 (moderate renal impairment) or serum creatinine concentration between 1.4 and 1.9mg/100mL, the maximum daily dose should be 1000mg for oral administration (all formulations) or 800mg for an intravenous regimen.
Patients with creatinine clearance less than 30mL/min/1.73m
2 (severe renal impairment) or serum creatinine concentration equal or higher than 2.0mg/100mL, the maximum daily dose should be 500mg for oral administration (all formulations) or 400mg for an intravenous regimen.
Children and adolescents: Dosing in children with impaired renal and or hepatic function has not been studied.
Duration of treatment: The duration of treatment depends on the severity of the illness and on the clinical and bacteriological course. It is essential to continue therapy for at least 3 days after disappearance of the fever or of the clinical symptoms. Mean duration of treatment: 1 day for acute uncomplicated gonorrhea and cystitis; up to 7 days for infections of the kidneys, urinary tract and abdominal cavity; over the entire period of the neutropenic phase in patients with weakened body defenses; a maximum of 2 months in osteomyelitis; and 7-14 days in all other infections.
In streptococcal infections, the treatment must last at least ten days because of the risk of late complications. Infections caused by Chlamydia should also be treated for a minimum of ten days.
Children and adolescents: Cystic Fibrosis: For broncho-pulmonary infections of cystic fibrosis associated with
Pseudomonas aeruginosa infection in pediatric patients (aged 5-17 years), the duration of treatment is 10-14 days.
Complicated Urinary Tract Infections and Pyelonephritis: For complicated urinary tract infections or pyelonephritis due to
Escherichia coli, the duration of treatment is 10-21 days.
Inhalational Anthrax (Post-exposure) in Adults and Children Adults: Oral administration: 500mg twice daily.
Children: Oral administration: 15mg/kg twice daily. The maximum of 500mg per dose should not be exceeded (maximum daily dose of 1000mg).
60 days from the confirmation of
Bacillus anthracis exposure.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
